No one concept has been so misunderstood confused and abused as that of ‘core control’. Fixing and bracing does not equate with movement control, nor does activation of transversus abdominus alone. I am continually perplexed by the number of clients I see whose training in ‘core stability’ is increasing their movement dysfunction and therefore their pain experience.
Hodges and Richardson’s research was fundamental in shifting the professions focus to the core. It demonstrated that there is reduced and delayed activation of transverse abdominus in people with back pain – this is now well understood. But, Hodges research also showed that control of the spine should be dynamic, and that stability equates to controlled mobility.
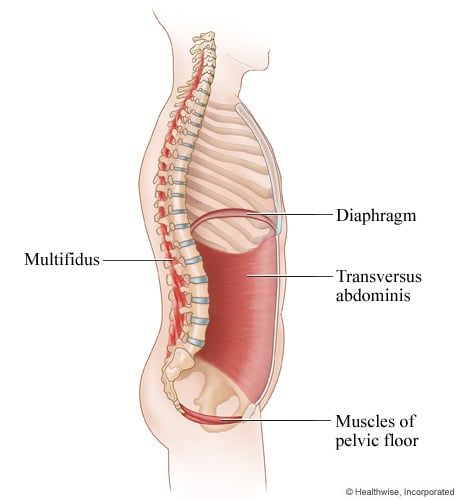
Critical to interpreting Hodges research is understanding normal spinal mechanics. Transversus abdominus contracts in conjunction with the pelvic floor, diaphragm and multifidus prior to actual movement, and as part of the postural reflex synergy – it does not act in isolation. This research demonstrates the importance of co-activation, breathing and functional control.
While single muscle activation of transversus abdominus using ultrasound may initially ‘help get the feel’ of the desired muscle activation, retraining needs to involve functionally relevant posturo-movement patterns that reinforce co-activation. Bracing, hollowing or drawing the belly button inwards in an effort to engage transversus abdominus and the pelvic floor limits the action of the diaphragm, thereby inhibiting functional stability. Bracing results in paradoxical breathing patterns and central holding patterns that often underlie a patient’s musculo-skeletal complaints.
Clinically we see that the first sign of defective core control is defective breathing patterns.
So why is breathing so important?
Stiffness in the lower pole of the thorax results from bracing and over engagement of the superficial muscles and compromises the downward descent of the diaphragm and resultant stability. To understand this, a clear picture of the stages of inspiration is required.
Stages of inspiration
- The diaphragm descends like a piston, resulting in expansion of the lower ribcage. This results in negative intra-thoracic pressure which draws air into the lungs. At the same time, the downward descent of the diaphragm results in positive intra-abdominal pressure.
- With a further increase in intra-abdominal pressure by increasing the lower diameter of the thorax, the diaphragm becomes part of the postural control mechanism resulting in increased intra-abdominal pressure. The descent of the diaphragm causes a co-activation of the pelvic floor. Intra-abdominal pressure thereby becomes the point of stability and contributes to postural support.
If breathing is defective, which usually coincides with functional adaptations to the fundamental patterns of movement, changing the way someone breathes can fundamentally their experience of their body, their pain and improve their functional control.
Retrain breathing to establish stability
Basic principals of retraining diaphragmatic breathing
- Breathe in through the nose and out through the mouth or nose
- Breathe low into the body, focus on expanding the entire lower pole of the rib cage. Relax the neck muscles
- Breathe slowly – a good ratio to work on is breathe in for a count of 2, out for 3 and pause for 1 second or more. A healthy rate of breathing is approximately 12-14 breaths per minute
- The breathe is low NOT big
- Stress or hyper-arousal leads to an increased rate and volume of the breath which engages the accessory muscles of breathing
- Once breathing is established in a static position progress to training the breath during functional movements
- TIP: Breath holding during ‘ordinary movement’ is a compensation for deficient posturo-movement control
- Breath holding with very strong effort actions/lifting (Valsalva = maximal IAP) reinforces postural control (Hemborg et al 1985) – and is ‘normal’
Slow down, breathe, feel your ribs expand and notice how good you feel.